What Makes Retatrutide a Triple Agonist
Retatrutide is a “triple agonist” because it activates three separate hormones simultaneously: GLP-1, GIP, and glucagon.
KEY TAKEAWAYS
- Retatrutide is called a “triple agonist” because it activates three hormone receptors at the same time: GLP-1, GIP, and glucagon (GCGR).
- Each receptor does a different job, reducing hunger, boosting insulin, and burning fat.
- No other approved weight loss drug currently targets all three of these receptors simultaneously.
- In Phase 2 clinical trials, retatrutide produced up to 24.2% body weight loss in 48 weeks, more than any other approved weight loss drug.
- Phase 3 data from December 2025 suggested average weight loss could reach 28–29%, rivaling bariatric surgery results.
- Retatrutide is developed by Eli Lilly (also known by its code name LY3437943) and is not yet FDA-approved as of mid-2026.
- Side effects are mostly gastrointestinal and are usually worst during dose increases.
What Makes Retatrutide a “Triple” Agonist?
If you’ve heard the buzz about retatrutide and wondered what makes it different from Ozempic or Mounjaro, the answer comes down to one key phrase: triple agonist.

Most weight loss drugs work by targeting a single hormone receptor in your body. Some newer ones, like tirzepatide (Mounjaro), target two. Retatrutide goes one step further, it targets three.
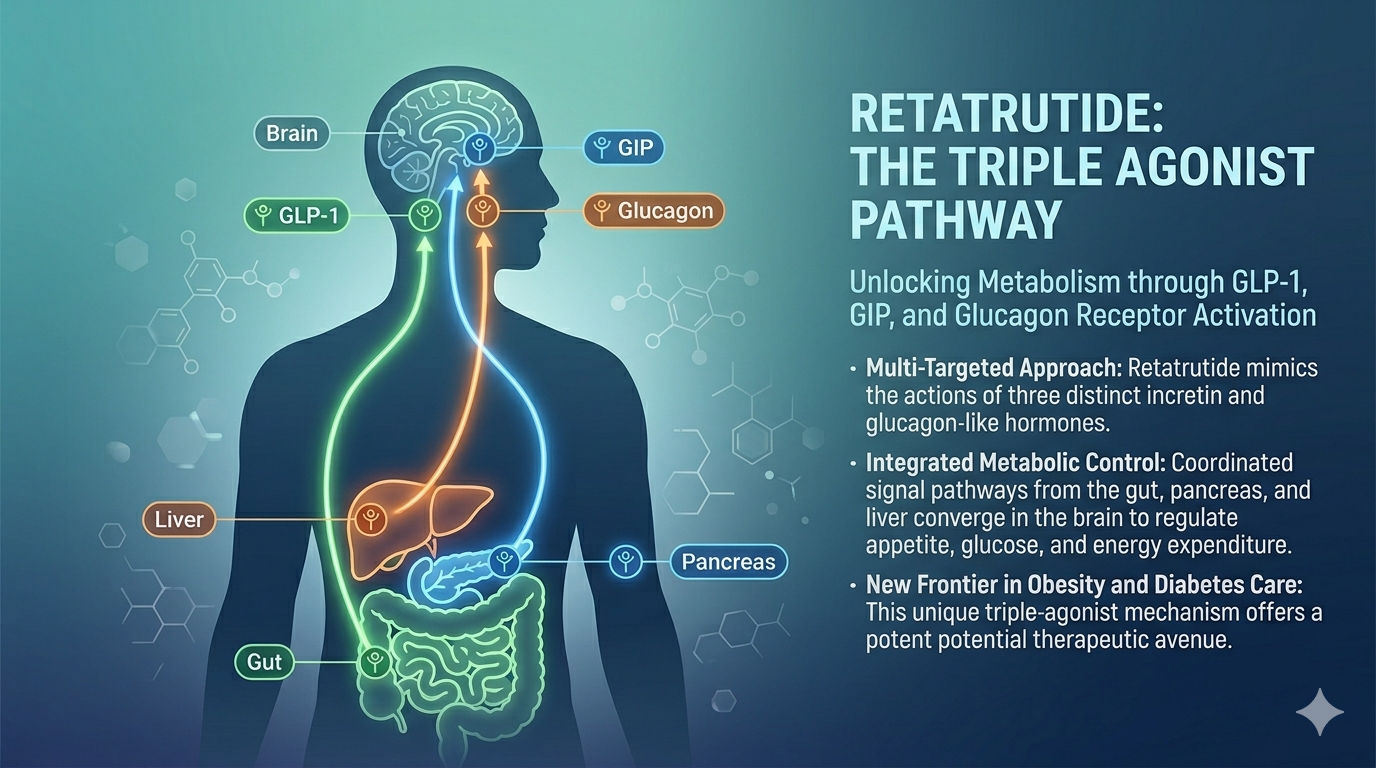
Specifically, retatrutide activates the GLP-1 receptor, the GIP receptor, and the glucagon receptor all at the same time. Because it activates (or “agonizes”) all three, scientists and researchers call it a triple agonist, or sometimes a “triagonist.”
Think of it like turning on three light switches instead of one or two. Each switch controls a different part of your metabolism, your appetite, your insulin response, and your body’s ability to burn fat. By flipping all three at once, retatrutide is designed to tackle obesity and type 2 diabetes more completely than previous drugs.
This article explains exactly what an agonist is, why having three matters, what each of the three receptors does in your body, and how they work together to produce the results seen in clinical trials.
What Is an Agonist?
Before we can understand why retatrutide is a triple agonist, we need to understand what an “agonist” actually means.
In simple terms, an agonist is a substance that activates a receptor in your body. Think of a receptor like a lock and an agonist like the matching key. When the key turns the lock, it triggers a chain reaction, a biological signal that tells your body to do something.
Your body makes its own natural agonists all the time. These are called hormones. For example, the hormone insulin is an agonist for insulin receptors. When insulin binds to its receptor, your cells open up and absorb sugar from your blood.
Drugs can act as agonists too. When a drug mimics a natural hormone and binds to the same receptor, it “turns on” the same biological response, sometimes even more powerfully or for longer than the natural hormone would.
So when we say retatrutide is a “triple agonist,” we mean it acts like a key that can fit three different locks at the same time, triggering three separate sets of biological actions with a single drug.
Types of Agonists in Metabolic Medicine
To understand where retatrutide fits, it helps to see how agonist-based drugs have evolved over time.
Single Agonists target one receptor. Semaglutide (Ozempic, Wegovy) is the most well-known example. It activates only the GLP-1 receptor. While it has been very effective, it only works through one pathway.
Dual Agonists target two receptors. Tirzepatide (Mounjaro, Zepbound) was a major step forward when it was approved in 2022 because it targets both GLP-1 and GIP receptors. This combination gave it stronger weight loss results than semaglutide alone.
Triple Agonists target three receptors at once. Retatrutide is the most advanced triple agonist currently in late-stage clinical trials. It adds glucagon receptor activation on top of what tirzepatide already does.
Each step up the ladder has produced better weight loss results, which is why the research community is watching retatrutide so closely.
The Three Receptors Retatrutide Targets
Here is a quick overview before we go into detail on each one:
| Receptor | Full Name | Main Role |
|---|---|---|
| GLP-1R | Glucagon-Like Peptide-1 Receptor | Reduces appetite, slows digestion, boosts insulin |
| GIPR | Glucose-Dependent Insulinotropic Polypeptide Receptor | Enhances insulin release, metabolic support |
| GCGR | Glucagon Receptor | Burns fat, increases energy use, targets liver fat |
Together, these three pathways cover appetite, blood sugar control, and fat burning, the three biggest challenges in treating obesity and type 2 diabetes.
The First Agonist of the Triple Agonist : GLP-1 Receptor Activation
What Is GLP-1?
GLP-1 stands for Glucagon-Like Peptide-1. It is a hormone your gut naturally releases after you eat. Its main job is to tell your body that food has arrived and help manage what happens next.
What Does GLP-1 Do in Your Body?
GLP-1 does several important things at once. It signals your pancreas to release insulin, but only when blood sugar is high, which makes it safe. Additionally, it tells your liver to slow down producing new sugar. It slows how fast your stomach empties, so you feel full longer. And it sends signals to the appetite center in your brain to reduce hunger.
In plain terms, GLP-1 is your body’s natural “put the fork down” signal.
How Does GLP-1 Receptor Activation Help With Weight Loss?
When retatrutide activates the GLP-1 receptor, people eat less because they feel satisfied sooner and stay full longer. They also have better blood sugar control because insulin is released at the right time.
This is the same mechanism that made semaglutide (Ozempic/Wegovy) famous. It is well-studied, well-understood, and proven to produce significant weight loss. The GLP-1 pathway is considered the backbone of modern obesity medication.
GLP-1 in Retatrutide vs. Other Drugs
In retatrutide, the GLP-1 receptor is activated with a potency (EC50) of about 0.775 nM. This is somewhat less potent than its action on the GIP receptor, but it still plays a central role in appetite reduction and blood sugar management.
The Second Agonist: GIP Receptor Activation
What Is GIP?
GIP stands for Glucose-Dependent Insulinotropic Polypeptide. Like GLP-1, it is also an incretin hormone, meaning it is released from your gut in response to food and helps manage insulin.
GIP is released from cells in the upper part of your small intestine (the duodenum and jejunum) shortly after you begin eating.
What Does GIP Do in Your Body?
GIP’s primary role is to boost insulin secretion from the pancreas after meals. It works alongside GLP-1 to make sure your blood sugar is handled quickly and efficiently. Research also shows that GIP plays a role in regulating fat storage in adipose tissue and has effects on bone metabolism.
One important difference from GLP-1 is that GIP can help protect against hypoglycemia (dangerously low blood sugar) by slightly raising glucagon when glucose levels drop too low, making the combination of GIP and GLP-1 quite balanced from a safety standpoint.
Why Adding GIP to GLP-1 Makes a Difference
When tirzepatide added GIP activation to GLP-1, patients lost more weight than with GLP-1 alone. Researchers believe GIP enhances the metabolic effects of GLP-1 and may reduce some of the side effects that come with GLP-1-only drugs.
GIP also acts on the brain’s satiety center, adding another layer of appetite control on top of GLP-1.
GIP in Retatrutide
Notably, retatrutide is actually most potent at the GIP receptor, with an EC50 of about 0.0643 nM, roughly ten times more potent here than at the GLP-1 receptor. This strong GIP activity is thought to contribute meaningfully to retatrutide’s weight loss results and may also help reduce gastrointestinal side effects compared to a drug that relied on GLP-1 alone at full strength.
The Third Agonist: Glucagon Receptor Activation
What Is Glucagon?
Glucagon is a hormone produced in the pancreas. It is GLP-1’s natural counterpart, while GLP-1 lowers blood sugar, glucagon raises it. When your blood sugar drops too low (like between meals or during exercise), your pancreas releases glucagon to tell your liver to release stored sugar.
But glucagon does more than just manage blood sugar. It is also a powerful regulator of fat metabolism and energy expenditure.
What Does Glucagon Receptor Activation Do?
When the glucagon receptor is activated, several important things happen. The liver breaks down stored fat (a process called lipolysis), releasing fatty acids to be used as fuel. The body increases its overall calorie burn, a process called thermogenesis. The liver reduces the buildup of fat in liver cells, which is important for treating fatty liver disease (MASLD). And glucagon signals the liver to produce energy through a process called gluconeogenesis.
In short, glucagon tells your body to burn fat and use stored energy — even at rest.
Why Glucagon Activation Was Avoided Before
Here is the catch: glucagon on its own raises blood sugar. That is a serious problem if you are treating type 2 diabetes. This is why earlier researchers were hesitant to include glucagon activation in diabetes or obesity drugs.
However, when glucagon receptor activation is paired with GLP-1 and GIP both of which lower blood sugar, the blood sugar-raising effect of glucagon is largely balanced out. The fat-burning and energy-spending benefits are kept, while the dangerous blood sugar spike is prevented.
This balancing act is one of the key innovations in retatrutide’s design.
The Liver Fat Connection
One of the most exciting findings about glucagon receptor activation is its effect on liver fat. A 2024 study published in Nature Medicine found that retatrutide produced significant reductions in liver fat in patients with metabolic dysfunction-associated steatotic liver disease (MASLD). The glucagon receptor pathway appears to directly drive the breakdown of fat stored in liver cells, something that GLP-1 alone cannot achieve as effectively.
How the Three Agonists Work Together
Each receptor does something useful on its own. But the real power of retatrutide comes from how all three work together as a coordinated system.
Here is a simple way to think about it:
GLP-1 receptor = puts the brakes on appetite and slows digestion. You eat less and feel full faster.
GIP receptor = amplifies the insulin response and adds another layer of satiety signaling. Blood sugar is managed more efficiently with fewer side effects.
Glucagon receptor = tells your body to burn existing fat stores and use more energy even when you’re not exercising.
Together: you eat less, your blood sugar is controlled, AND your body burns more fat simultaneously. That is a three-front attack on obesity that no single or dual agonist can match.
Researchers describe this as “inter-organ crosstalk”, retatrutide signals the pancreas, brain, liver, and fat tissue all at once to create a coordinated metabolic improvement. The liver processes fat better, the pancreas releases insulin more precisely, the brain sends less hunger signals, and fat stores shrink.
This explains why clinical trial results have been so striking. In a Phase 2 trial published in the New England Journal of Medicine, participants taking the highest dose (12 mg weekly) lost an average of 24.2% of their body weight over 48 weeks. Phase 3 data reported in December 2025 pointed to average losses of 28–29%, a figure that rivals the results of bariatric surgery.
Retatrutide vs. Other Weight Loss Drugs: How It Compares
| Drug | Receptor(s) Targeted | Average Weight Loss | FDA Approved? |
|---|---|---|---|
| Semaglutide (Wegovy) | GLP-1 only | ~15% | Yes (2021) |
| Tirzepatide (Zepbound) | GLP-1 + GIP | ~20–22% | Yes (2023) |
| Retatrutide | GLP-1 + GIP + Glucagon | ~24–29% | Not yet (Phase 3) |
The progression is clear. Each additional receptor target has produced meaningfully stronger results.
What Conditions Could Retatrutide Treat?
Because retatrutide affects so many metabolic pathways, it is being studied for more than just weight loss. Current Phase 3 trials, known as the TRIUMPH studies, are evaluating retatrutide for:
Obesity — the primary indication, with Phase 3 results showing up to 28–29% weight loss.
Type 2 Diabetes– the triple mechanism produces potent glucose regulation. The GLP-1 receptor drives insulin release, the GIP receptor amplifies it, and the glucagon receptor’s effects on blood sugar are carefully counterbalanced.
Metabolic dysfunction-associated steatotic liver disease (MASLD)– formerly called NAFLD. The 2024 Nature Medicine trial showed significant liver fat reduction.
Knee osteoarthritis in people with obesity– Phase 3 trials are also evaluating whether weight loss from retatrutide reduces joint pain.
Common Misconceptions About Triple Agonist
Misconception 1: “It’s just a stronger Ozempic.”
Not quite. Ozempic (semaglutide) only activates the GLP-1 receptor. Retatrutide activates two additional receptors — GIP and glucagon — which involve completely different biological pathways. The result is not just “more of the same” but a fundamentally different metabolic effect, particularly through the fat-burning and liver-targeting properties of glucagon receptor activation.
Misconception 2: “The glucagon part will spike my blood sugar dangerously.”
This was a valid concern when glucagon was studied alone. But in retatrutide, the GLP-1 and GIP components produce enough insulin-stimulating activity to counterbalance glucagon’s blood sugar-raising effect. Clinical trials have not shown dangerous blood sugar spikes — in fact, diabetic participants saw significant HbA1c reductions.
Misconception 3: “You can buy retatrutide online right now.”
As of mid-2026, retatrutide is NOT FDA-approved. The only legal way to receive it is within a clinical trial. The FDA has explicitly warned against compounded or unapproved versions sold online, which carry serious safety risks due to unknown purity and dosing.
Misconception 4: “Side effects are completely different from other GLP-1 drugs.”
The most common side effects — nausea, diarrhea, vomiting, and constipation — are very similar to those seen with semaglutide and tirzepatide. They are dose-dependent and tend to be worst during dose increases, then improve as the body adjusts.
Misconception 5: “Triple agonist means triple the side effects.”
Clinical trial data does not support this. While side effects do increase with dose, the addition of GIP activation may actually help reduce some GLP-1-related side effects. Serious adverse events in Phase 2 trials were rare and comparable to placebo.
What Are the Side Effects of Triple Agonist?
Based on Phase 2 and Phase 3 (TRIUMPH-4) clinical trial data, the most commonly reported side effects are:
Gastrointestinal effects are the most frequent. Nausea affects a significant portion of participants, especially at higher doses — up to 43% at 12 mg in Phase 3 data. Diarrhea, constipation, and vomiting follow similar patterns. These effects are typically most intense during dose escalation and tend to improve once a stable dose is reached.
Increased heart rate — some participants at higher doses experienced a modest rise of about 5–7 beats per minute, which trended back toward normal by weeks 36–48.
Skin sensitivity — a unique finding sometimes seen with the glucagon receptor component; tingling or altered skin sensation was reported in some participants at higher doses.
Hair thinning — sometimes seen with rapid weight loss in general, not specific to retatrutide.
Serious adverse events such as pancreatitis and gallbladder events were rare in Phase 2, occurring at similar rates to placebo. Long-term safety is still being evaluated in ongoing Phase 3 trials.
The Science Behind Triple Agonist Design
Retatrutide was engineered as a single continuous molecule — not a mixture of three separate drugs. Its molecular structure forms a helix that allows it to bind to all three receptor types.
Structurally, retatrutide’s N-terminal segment (the front end of the molecule) interacts with the core of each receptor’s transmembrane domain. Its C-terminal segment (the back end) interacts with the outer portions of each receptor. This dual-end engagement is what allows one molecule to successfully activate three different receptors.
The molecule is also acylated — meaning a fatty acid chain is attached to it — which extends its half-life in the bloodstream and allows for once-weekly dosing, just like semaglutide and tirzepatide.
What Does the Research Say? Clinical Trial Overview
Phase 2 Trial (New England Journal of Medicine, 2023) A randomized, double-blind, placebo-controlled trial in adults with obesity (without type 2 diabetes) showed:
- 24.2% average weight loss at 48 weeks (12 mg dose)
- 22.8% average weight loss at 8 mg
- Over 90% of participants achieved at least 5% weight loss
- Significant improvements in blood pressure, waist circumference, and cardiometabolic markers
Phase 2a Liver Study (Nature Medicine, 2024) A substudy specifically in patients with metabolic dysfunction-associated steatotic liver disease showed statistically significant reductions in liver fat content, particularly with the glucagon receptor component driving hepatic lipid oxidation.
TRIUMPH Program, ongoing Multiple Phase 3 trials (the TRIUMPH studies) are underway. In December 2025, Eli Lilly reported Phase 3 topline data from TRIUMPH-4, suggesting average weight loss of approximately 28–29% over 68 weeks — a figure that would make retatrutide the most effective obesity drug ever developed without surgery.
FDA approval is estimated for late 2026 to early 2027, pending full trial data review.
Final Thoughts
Retatrutide is called a triple agonist because it does what no approved weight loss drug currently does: it activates three different hormone receptors — GLP-1, GIP, and glucagon — simultaneously with a single injection.
Each receptor contributes something the others cannot fully replicate. GLP-1 curbs your appetite and slows digestion. GIP amplifies insulin release and adds metabolic synergy. Glucagon tells your liver and fat tissue to burn stored energy.
When all three work together, the result is a level of weight loss that rivals bariatric surgery — without going under the knife.
The science behind retatrutide is not hype. It is built on years of incremental research, from single to dual to triple receptor targeting, with clinical trials at every step confirming that more receptors targeted means better results.
Whether retatrutide will eventually join the pharmacy shelf alongside Ozempic and Mounjaro remains to be confirmed by the FDA. But based on the evidence available, it represents the most advanced pharmacological approach to obesity ever developed.
Frequently Asked Questions (FAQs)
What does “triple agonist” mean in simple terms?
It means retatrutide acts like a key that fits three different biological locks (receptors) in your body at the same time. Each lock, when opened, triggers a different weight-loss or metabolic benefit.
How is retatrutide different from Ozempic?
Ozempic (semaglutide) only activates the GLP-1 receptor. Retatrutide activates two more — the GIP receptor and the glucagon receptor — adding fat-burning and energy-expenditure effects that semaglutide cannot provide.
How is retatrutide different from Mounjaro (tirzepatide)?
Tirzepatide is a dual agonist targeting GLP-1 and GIP. Retatrutide adds a third target — the glucagon receptor — which increases fat burning and appears to have specific benefits for liver fat. Clinical trials suggest this third target produces meaningfully greater weight loss.
Is retatrutide FDA-approved?
A: No. As of mid-2026, retatrutide is still in Phase 3 clinical trials. It is not approved or legally available outside of clinical research. FDA approval is estimated for late 2026 to early 2027.
Will retatrutide raise my blood sugar because it activates glucagon?
Clinical trials have not shown this to be a problem. The GLP-1 and GIP components of retatrutide counterbalance glucagon’s blood sugar-raising effect, and diabetic participants in trials actually saw significant reductions in HbA1c.
How much weight can you lose with retatrutide?
Phase 2 trials showed up to 24.2% body weight loss at 48 weeks. Phase 3 data (December 2025) suggested 28–29% average weight loss over 68 weeks at higher doses. Results vary by individual, dose, and adherence.
What are the most common side effects of Retatrutide?
A: Nausea, diarrhea, vomiting, and constipation — the same gastrointestinal effects seen with other GLP-1-based medications. They are usually worst during dose increases and tend to improve over time.
Who makes retatrutide?
A: Retatrutide is developed by Eli Lilly and Company. Its research code name is LY3437943.
Does retatrutide help with liver disease?
A: Early research is promising. A 2024 Nature Medicine study found significant liver fat reductions in patients with MASLD (metabolic dysfunction-associated steatotic liver disease), largely attributed to the glucagon receptor component of the drug.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. Retatrutide is an investigational drug and is not FDA-approved. Consult a qualified healthcare provider for guidance on any medical treatment.
Leave a Reply